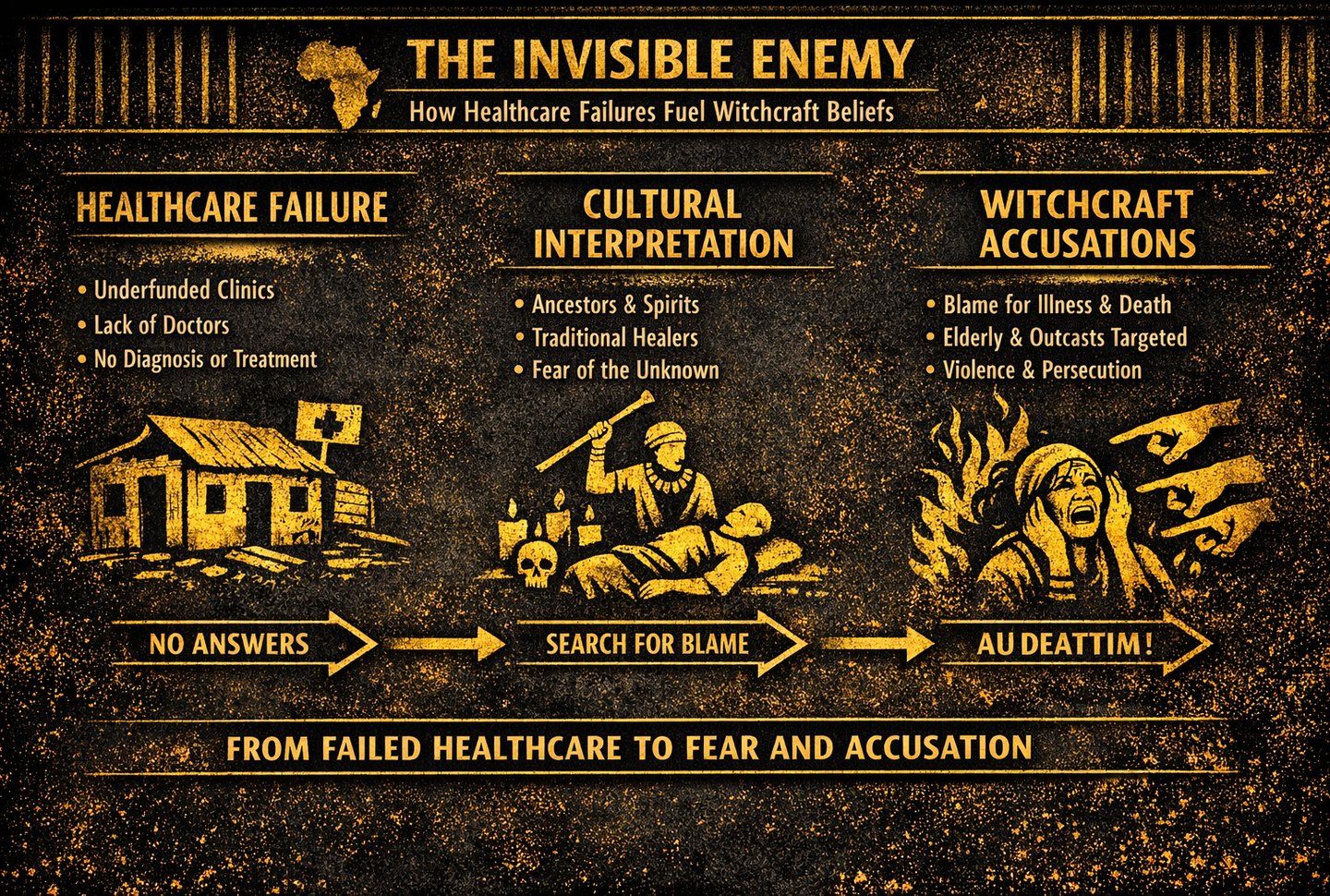
The Invisible Enemy: How Africa’s Broken Healthcare System Fuels Belief in Witchcraft
A critical examination of the structural failures in African healthcare, from underfunded clinics to chronic shortages of trained workers, and how these gaps create the conditions where preventable deaths and witchcraft accusations thrive.
enoma ojo (2024)
1/24/202610 min read


This is the Story of Two Lives, One World, and a Healthcare System That Decides Who Survives
In Houston, Texas, 42‑year‑old Michael woke up one morning with a crushing pain in his chest. His wife immediately dialed 911. Within minutes, paramedics arrived, connected him to oxygen, ran an ECG, and rushed him to a fully equipped emergency room. Doctors diagnosed a heart attack, opened his blocked artery, and stabilized him. By evening, he was awake, exhausted but alive. His cardiologist told him, “You came in just in time. You’re going to recover.”
In Benue State, in Middle-Belt Nigeria, 39‑year‑old Terfa woke up with the same chest pain. His wife panicked, but there was no emergency number to call. Neighbors carried him on a motorcycle to the nearest clinic. There was no doctor on duty, no ECG machine, and no oxygen. The nurse gave him paracetamol and advised them to try a bigger hospital in the next town. By the time they found a car, Tunde was unconscious. He died on the way.
His family, devastated and confused, concluded that someone must have bewitched him. “This was not ordinary,” they said. “Someone did this to him.” “Village people again?”
Two men. Two families. Two identical medical emergencies.
But two completely different outcomes, not because of fate, not because of witchcraft, but because of the systems surrounding them.
Michael survived because his environment gave him a chance, and Terfa died because his environment did not, and in the absence of answers, his community turned to the explanations they have always known. This is not a story about superstition.
It is a story about a healthcare system so broken that people must fill the gaps with whatever explanations they can find.
In many African societies, illness is rarely viewed as a purely biological event. When someone falls sick suddenly or mysteriously, the first explanations often come from cultural and spiritual traditions that have existed for centuries. These beliefs are not rooted in ignorance but in history. Long before modern hospitals existed, communities relied on traditional healers, spiritual leaders, and ancestral wisdom to understand sickness. Today, these beliefs persist not simply because they are cultural, but because the healthcare system in many African countries is deeply broken, underfunded, and inaccessible to millions.
When hospitals lack doctors, clinics lack medicine, and diagnostic tools are unavailable, people naturally turn to explanations that feel more reliable than a system that repeatedly fails them. In rural areas, some communities must travel 20 to 50 kilometers to reach the nearest health facility. For many, the journey is too long, too expensive, or too dangerous, especially during emergencies. Even when patients reach a clinic, they often encounter long queues, overwhelmed nurses, and empty pharmacies. The absence of care creates a vacuum that superstition quickly fills. Diseases like hypertension, diabetes, kidney failure, and stroke often progress silently. Without proper testing, they appear sudden and mysterious, reinforcing the belief that unseen forces are at work. Statistics show that over 70% of hypertension cases in sub‑Saharan Africa go undiagnosed, and more than 60% of diabetes cases are discovered only after complications arise.
When someone collapses or becomes paralyzed overnight, families interpret it as witchcraft because the medical system never gave them the tools to understand the illness. Poverty further deepens the problem. In many African countries, over 40% of healthcare expenses are paid out-of-pocket, making treatment unaffordable for millions. Faced with high costs, people turn to traditional healers, prayer houses, and spiritualists, not because they prefer them, but because they are accessible, affordable, and culturally familiar. Mental health is another area where the system fails dramatically. Africa has one of the lowest psychiatrist-to-population ratios in the world, with some countries having fewer than ten psychiatrists nationwide. Conditions like epilepsy, schizophrenia, and severe depression are often labeled as curses, possession, or spiritual attacks because there is no medical language or support available to explain them. Families often resort to chaining, isolating, or taking mentally ill relatives to spiritual camps because they believe they are fighting a supernatural force, not a medical condition. The lack of trust in hospitals is also fueled by repeated tragedies. When people die from treatable conditions due to a lack of oxygen, blood, or antibiotics, communities lose faith in modern medicine.
In Africa, the line between illness and the supernatural is not simply cultural; it is structural. When clinics are understaffed, hospitals lack basic equipment, and emergency care is hours away, people turn to the explanations that feel closest, most accessible, and most emotionally coherent. In the absence of a functioning healthcare system, witchcraft becomes the language through which suffering is interpreted, and the invisible enemy becomes easier to name than the systemic failures that created the crisis. For millions, sickness is not just a biological event; it is a social and spiritual disruption. A child convulsing from untreated malaria, a woman dying from postpartum hemorrhage because the nearest facility has no blood, a man losing his mind from undiagnosed meningitis, these are not seen as medical tragedies but as spiritual attacks. When the system cannot diagnose, cannot treat, and cannot save, communities fill the vacuum with explanations that offer meaning, agency, and someone to blame.
This belief is not born from ignorance; it is born from abandonment. When governments underfund primary care, when rural clinics run without electricity, when patients must pay out‑of‑pocket for basic drugs, people naturally seek answers elsewhere. Witchcraft becomes a coping mechanism in a world where science is present in theory but absent in practice. The supernatural becomes the default when the state is missing. Yet beneath the cultural narrative lies a deeper truth: the real enemy is not the witch in the village but the broken system that leaves people to die from preventable diseases. The real “curse” is the lack of infrastructure, the shortage of trained health workers, the corruption that diverts medical supplies, and the decades of policy neglect that have normalized avoidable deaths. Witchcraft thrives not because people reject modern medicine, but because modern medicine has rejected them.
Across many African societies, culture and tradition serve as powerful organizing forces, shaping identity, community, and meaning. But these same systems can also influence how people interpret illness, misfortune, and death, especially in contexts where formal institutions are weak. When healthcare systems fail to diagnose or treat common conditions, cultural explanations often fill the vacuum. This dynamic does not arise from ignorance, but from necessity: people rely on the frameworks available to them when the state cannot provide answers.
In regions where clinics lack equipment, trained personnel, or basic diagnostic tools, unexplained symptoms become fertile ground for spiritual interpretations. A child convulsing from untreated malaria, a woman dying from postpartum hemorrhage, or a man losing consciousness from undiagnosed hypertension — these events are often interpreted through cultural lenses. Without medical clarity, communities turn to ancestral beliefs, spiritual causation, or witchcraft to explain what the healthcare system cannot.
This reliance on traditional explanations is not inherently harmful; in many cases, traditional healers provide emotional support, community cohesion, and accessible care. The problem emerges when cultural interpretations replace medical intervention, especially for conditions that are preventable or treatable. When a fever is seen as a curse rather than an infection, or when mental illness is interpreted as a spiritual attack rather than a neurological condition, individuals lose precious time, and sometimes their lives.
Cultural beliefs also shape how communities respond to illness. In some regions, families may hide symptoms out of fear of stigma, witchcraft accusations, or social exclusion. This secrecy delays treatment and increases mortality. In other cases, communities may blame vulnerable individuals, elderly women, children, and widows for unexplained deaths, reinforcing cycles of violence and social fragmentation. These patterns thrive in environments where the healthcare system cannot provide authoritative explanations.
Tradition also influences gender roles, which in turn affect health outcomes. In many communities, women require permission from husbands or elders to seek care, delaying treatment for childbirth complications or chronic illnesses. Cultural norms may discourage men from seeking help due to expectations of strength and stoicism. These gendered expectations, deeply rooted in tradition, contribute to preventable deaths and untreated conditions.
Belief systems also shape trust, or mistrust, in modern healthcare. Historical experiences with colonial medicine, exploitative research practices, or government neglect have left some communities skeptical of hospitals and clinics. When cultural memory associates formal healthcare with danger or disrespect, people naturally turn to traditional healers who speak their language, share their worldview, and treat them with dignity. This mistrust becomes a barrier to vaccination, early diagnosis, and preventive care. At the same time, culture can be a powerful driver of progress when aligned with development goals. Community-based health workers, traditional birth attendants, and local leaders often play critical roles in bridging the gap between modern medicine and cultural expectations. When health interventions respect cultural norms, rather than dismiss them, adoption rates increase dramatically. The challenge is not to erase tradition, but to integrate it into a functional health ecosystem.
However, the persistence of witchcraft accusations reveals a deeper structural issue: the absence of reliable institutions. In societies where the state cannot guarantee safety, justice, or healthcare, people rely on informal systems of explanation and accountability. Witchcraft becomes a way to assign blame, restore order, or make sense of tragedy. These beliefs flourish not because culture is static, but because institutions are weak. The impact on development is profound. When illness is misinterpreted, when fear replaces diagnosis, and when communities turn inward rather than toward evidence-based care, progress slows. Children miss school due to preventable diseases, adults lose productivity, and families spend scarce resources on ineffective treatments. The economic cost of these cultural and institutional gaps is enormous, measured not only in money but in lost potential.
Ultimately, Africa’s cultural and traditional systems are not obstacles to development in themselves. They become obstacles only when they operate in a vacuum created by failing institutions. Strengthening healthcare systems, improving education, and building trust in public services can transform cultural beliefs from barriers into assets. When people have access to reliable information, dignified care, and functioning institutions, harmful interpretations fade, and culture becomes a foundation for progress rather than a refuge from systemic failure.
This investigation exposes how fragile health systems shape belief, how belief shapes behavior, and how behavior shapes outcomes. It is a story about culture, yes, but more importantly, it is a story about systems, power, and the human need for explanations when institutions fail. To understand the persistence of witchcraft accusations, we must first confront the deeper, more uncomfortable truth: Africa’s healthcare crisis is not just medical. It is psychological, cultural, and profoundly political. Sub‑Saharan Africa and South Asia together account for over 80% of global under‑five deaths. In 2021, West and Central Africa alone recorded 1.89 million under‑five deaths, the highest regional burden globally. Africa continues to experience extremely high mortality from diseases that are treatable or preventable with basic healthcare. Across all age groups, preventable deaths in Africa are driven by: Weak primary healthcare systems, shortages of trained health workers, stock‑outs of essential medicines, long distances to facilities, high out‑of‑pocket costs, conflict and displacement, and low vaccination coverage. Non-communicable diseases accounted for 37% of all deaths in the WHO African region in 2019, up from 24% in 2000. Premature non-communicable deaths, between the ages of 30 and 70, in Africa are 63.6%, far above the global average of 41.8%. These systemic failures create conditions where avoidable deaths become normalized.
During crises like the COVID‑19 pandemic, oxygen shortages and overwhelmed hospitals led many to believe that deaths were caused by witchcraft or conspiracies rather than systemic failure. Traditional beliefs themselves are not the enemy. They are part of Africa’s cultural identity. The problem arises when these beliefs become the default medical system because the real one is collapsing. If healthcare were reliable, affordable, and well-equipped, people would naturally shift toward medical explanations and away from supernatural ones. Communities trust what works. When hospitals save lives consistently, belief in witchcraft as a cause of illness declines. When hospitals fail, spiritual explanations rise. Ultimately, the persistence of witchcraft explanations is not a cultural flaw but a symptom of a healthcare system that has not earned the trust of the people it is meant to serve.
Africa does not suffer from a superstition problem; it suffers from a healthcare crisis. People turn to witchcraft not because they reject science, but because the healthcare system rejects them. When hospitals lack medicine, when diagnoses are delayed, when emergencies go unanswered, and when preventable deaths become normal, communities seek answers wherever they can find them. If Africa wants to break the cycle of fear, suspicion, and spiritual blame, it must first fix the system that leaves millions without care. Because when healthcare becomes reliable, witchcraft becomes unnecessary, and when medicine finally works, the myths lose their power.
In the end, the tragedy of preventable deaths in Africa is not a mystery of culture but a failure of systems. People do not die because they lack belief in medicine; they die because medicine is too far, too expensive, too understaffed, or too broken to reach them. When institutions fail, explanations shift toward the supernatural, not because communities reject science, but because science has not shown up for them in any meaningful or reliable way. The real “invisible enemy” is not witchcraft, curses, or unseen forces. It is the quiet violence of neglect: the clinic without electricity, the hospital without oxygen, the ambulance that never comes, the health worker stretched beyond human limits. These are the forces that turn ordinary illnesses into fatal events and force families to seek meaning in the only frameworks available to them, and until African health systems become strong enough to offer timely, dignified, and accessible care, belief in witchcraft will continue to fill the vacuum left by institutional absence. And preventable deaths, the most unforgivable category of all, will remain a daily reality. The challenge before us is not to change culture, but to build systems worthy of the people they are meant to serve.
References
1. Global Health Workforce Alliance. (2015). A universal truth: No health without a workforce. World Health Organization.
2. Konadu-Yeboah, D., et al. (2020). Preventable trauma deaths and corrective actions: A 10-year study in Ghana. World Journal of Surgery, 44, 3643–3650.
3. Nguyen, H., & Peschka, M. (2017). The silent burden: Health system failures and cultural coping mechanisms in Africa. Brookings Institution.
4. Owusu, E. S. (2021). The superstition that maims the vulnerable: Witchcraft-driven mistreatment in Ghana. International Annals of Criminology, 58(2). Cambridge University Press.
5. Pfeiffer, J., & Nichter, M. (2008). What’s wrong with global health partnerships? A critical review. Social Science & Medicine, 67(5), 698–710.
6. The World Bank. (2022). Tracking universal health coverage in Africa. World Bank Publications.
7. UNICEF. (2021). Health systems bottleneck analysis in sub-Saharan Africa. UNICEF.
8. van den Broek, N., & Graham, W. (2009). Quality of care for maternal and newborn health: The neglected agenda. BJOG: An International Journal of Obstetrics & Gynaecology, 116(1), 18–21.
9. World Health Organization. (2023). State of health systems in Africa: Infrastructure, workforce, and access. WHO Regional Office for Africa.
10. Enoma Ojo. (2026). The Invisible Enemy: How Africa’s Broken Healthcare System Fuels Belief in Witchcraft. Inquiry & Insight.
© 2026 Inquiry & Insight by Enoma Ojo. All rights reserved. No part of this publication may be reproduced without permission.